
SCAD Beyond the Crisis: Predicting a Future of Personalized Cardiac Care for Women
Nearly 6-10% of heart attacks occur in women under 50, and a surprisingly large proportion are caused not by the typical plaque buildup, but by Spontaneous Coronary Artery Dissection (SCAD). This often-missed diagnosis, where a tear forms in a coronary artery wall, is now the focus of intensified research, and the implications extend far beyond current treatment protocols. We’re on the cusp of a revolution in how we understand, diagnose, and – crucially – prevent SCAD, particularly in the rising number of affected women.
The SCAD Puzzle: Why Younger Women Are Disproportionately Affected
For decades, heart disease was considered a ‘man’s disease.’ This bias led to underdiagnosis and delayed treatment for women experiencing atypical heart attack symptoms. SCAD further complicates this picture. Unlike atherosclerosis-driven heart attacks, SCAD often occurs in women with no traditional risk factors – normal cholesterol, no smoking history, and no hypertension. This makes it a particularly insidious condition, often misdiagnosed as anxiety or other less serious ailments.
Recent data from the European Society of Cardiology, as highlighted by Medical Xpress, reinforces this trend. The challenge lies in understanding why this is happening. Emerging research points to a complex interplay of hormonal factors, fibromuscular dysplasia (FMD – a condition affecting artery walls), and potentially, genetic predispositions.
The Role of Fibromuscular Dysplasia (FMD)
FMD is frequently found in SCAD patients, with estimates suggesting a co-occurrence rate of up to 80%. FMD causes abnormal cell growth in the artery walls, making them weaker and more susceptible to dissection. However, FMD itself is often overlooked, requiring specialized imaging techniques for diagnosis. The connection between FMD and SCAD is a critical area of ongoing investigation.
The Future of SCAD Diagnosis: AI and Advanced Imaging
Current diagnostic methods – angiography – are invasive and don’t always reveal the subtle tears characteristic of SCAD. The future of SCAD diagnosis lies in non-invasive techniques powered by artificial intelligence. AI algorithms are being trained to analyze cardiac MRI and CT angiography images with unprecedented accuracy, identifying early signs of arterial wall abnormalities and predicting the risk of dissection.
Imagine a scenario where routine cardiac screenings, coupled with AI-powered image analysis, can identify women at high risk of SCAD before a heart attack occurs. This proactive approach could dramatically reduce morbidity and mortality.
Genetic Screening: Unlocking Predispositions
The search for genetic markers associated with SCAD is gaining momentum. While no single ‘SCAD gene’ has been identified, researchers are uncovering variations in genes related to connective tissue, inflammation, and arterial wall integrity that may increase susceptibility. In the next decade, we can anticipate the development of genetic screening panels that assess an individual’s risk profile, allowing for personalized preventative strategies.
Personalized Prevention: A Paradigm Shift in Cardiac Care
The current treatment for SCAD is largely conservative – managing symptoms with medication and lifestyle changes. However, this approach doesn’t address the underlying cause. The future of SCAD management will be centered around personalized prevention, tailored to an individual’s risk factors.
This could include:
- Hormone therapy adjustments: For women with hormonal fluctuations linked to SCAD, carefully managed hormone therapy may play a role.
- Targeted medication: Drugs that strengthen artery walls or reduce inflammation could be prescribed based on genetic and imaging findings.
- Lifestyle modifications: Stress management techniques, tailored exercise programs, and dietary interventions will be crucial components of a preventative plan.
Furthermore, increased awareness among healthcare professionals is paramount. Educating doctors about the unique presentation of SCAD in women is essential for reducing diagnostic delays and improving outcomes.
| Metric | Current Status (2024) | Projected Status (2034) |
|---|---|---|
| SCAD Diagnostic Accuracy | 60-80% (Angiography) | 90-95% (AI-Enhanced Imaging) |
| Genetic Risk Prediction | Limited | Moderate – Identifying key gene variations |
| Preventative Treatment Options | Primarily Conservative | Personalized, Targeted Therapies |
Frequently Asked Questions About SCAD
What are the early warning signs of SCAD?
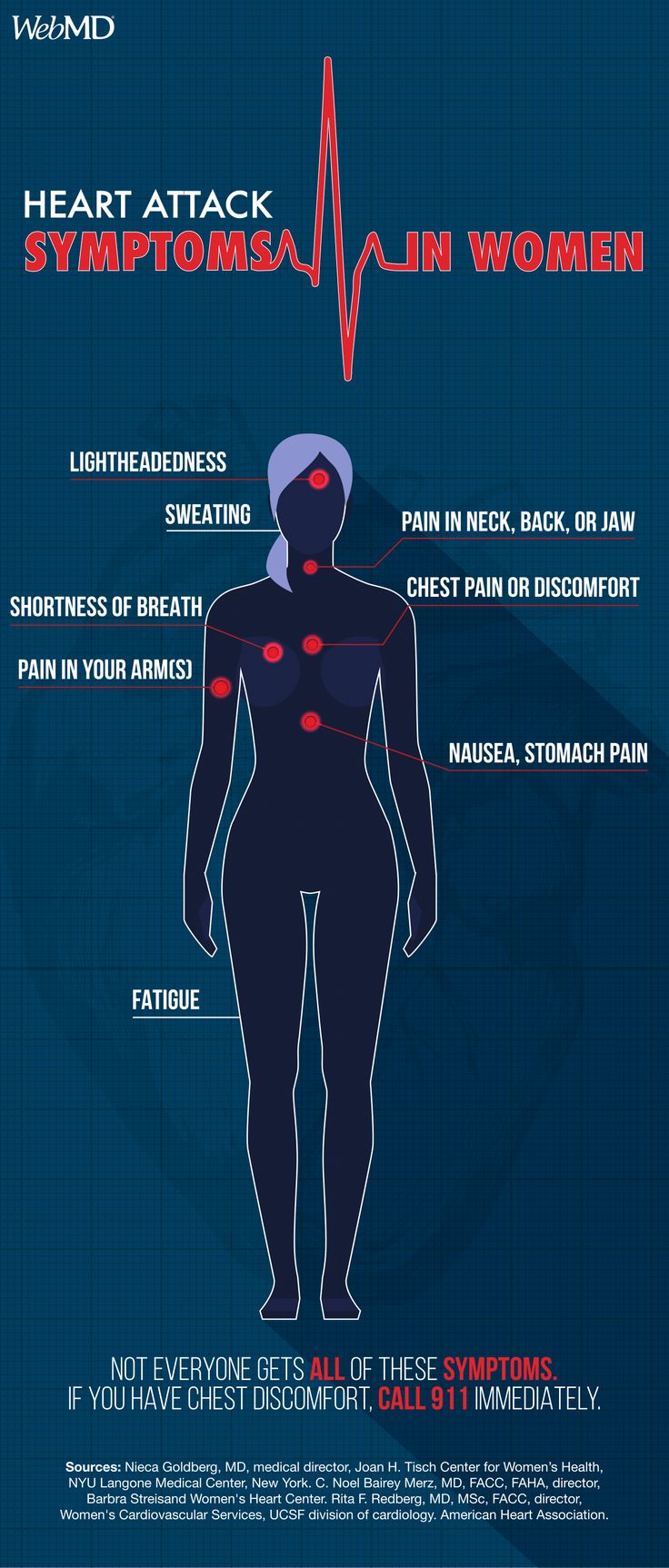
Symptoms can mimic a typical heart attack – chest pain, shortness of breath, nausea – but may be less severe and more intermittent. It’s crucial to seek immediate medical attention for any unexplained chest discomfort, especially if you have risk factors for FMD or a family history of SCAD.
Will SCAD happen again if I’ve had it once?
There is a risk of recurrence, estimated to be around 10-20%. However, with personalized preventative strategies and close monitoring, the risk can be significantly reduced.
Is SCAD related to pregnancy?
SCAD is more common during the peripartum period (late pregnancy and shortly after childbirth) due to hormonal changes and increased blood volume. Pregnant women experiencing chest pain should be evaluated immediately.
The future of SCAD care isn’t just about treating a crisis; it’s about predicting, preventing, and personalizing cardiac care for women. As our understanding of this complex condition deepens, we move closer to a world where SCAD is no longer a silent threat, but a manageable risk.
What are your predictions for the future of SCAD diagnosis and treatment? Share your insights in the comments below!
Discover more from Archyworldys
Subscribe to get the latest posts sent to your email.