Repurposing Existing Drugs: A New Frontier in Glioblastoma Treatment
Glioblastoma, the most aggressive form of brain cancer, has long defied effective treatment. But a paradigm shift is underway, fueled by the realization that the next breakthrough might not lie in developing entirely new drugs, but in cleverly redeploying those already approved for other conditions. Two “window-of-opportunity” Phase 2 clinical trials at Cleveland Clinic are now investigating this very concept, offering a glimmer of hope for patients facing this devastating diagnosis.
The Promise of Drug Repurposing in Glioblastoma
The conventional drug development process is notoriously lengthy and expensive. Drug repurposing, also known as drug repositioning, bypasses much of this, leveraging existing safety data and established manufacturing processes. This dramatically accelerates the timeline for potential new therapies, a critical advantage when dealing with a rapidly progressing disease like glioblastoma. Cleveland Clinic’s approach, led by Dr. David Peereboom, focuses on exploiting vulnerabilities within the tumor microenvironment and bolstering the body’s own immune defenses.
Methimazole: Boosting Hydrogen Sulfide to Combat Tumor Growth
The first trial (NCT05607407) centers on methimazole, a drug commonly used to treat hyperthyroidism. Researchers discovered a surprising link between hypothyroidism and increased production of hydrogen sulfide (H2S). Interestingly, H2S has been shown to inhibit the growth of glioblastoma cells in laboratory settings and slow tumor progression in animal models. Human brain tissue analysis further revealed lower H2S levels in glioblastoma compared to healthy brain tissue.
Rather than directly administering H2S – which presents logistical challenges – the team opted to stimulate its endogenous production. Methimazole proved effective in safely increasing H2S levels. Early results from the 15 patients enrolled so far are encouraging: a threefold rise in plasma H2S production was observed, alongside a progression-free survival rate of 15% at six months – exceeding expectations based on standard treatment. While overall survival at 12 months remained consistent with standard care, the preliminary efficacy signals are prompting plans for a larger, more comprehensive trial.
Sitagliptin: Unleashing the Immune System Against Glioblastoma
The second trial (NCT07003542) investigates sitagliptin, a medication used to manage type 2 diabetes. This approach tackles glioblastoma from a different angle: the immunosuppressive tumor microenvironment. Glioblastoma cells are adept at suppressing the immune system, allowing them to evade detection and destruction by immune cells. A key player in this suppression is myeloid-derived suppressor cells (MDSCs).
Previous research from Cleveland Clinic demonstrated that reducing MDSC levels can enhance immune infiltration of tumors, improving the effectiveness of existing therapies. Sitagliptin, a DPP-4 inhibitor, has shown promise in preclinical models for reducing circulating MDSCs with minimal toxicity. The current trial, involving 48 patients randomized to receive pre- and postoperative sitagliptin or postoperative sitagliptin alone, aims to determine if reducing MDSCs can enhance the efficacy of standard chemotherapy by boosting the number of CD8+ T cells within the tumor.
The Role of Radiomics in Personalized Treatment
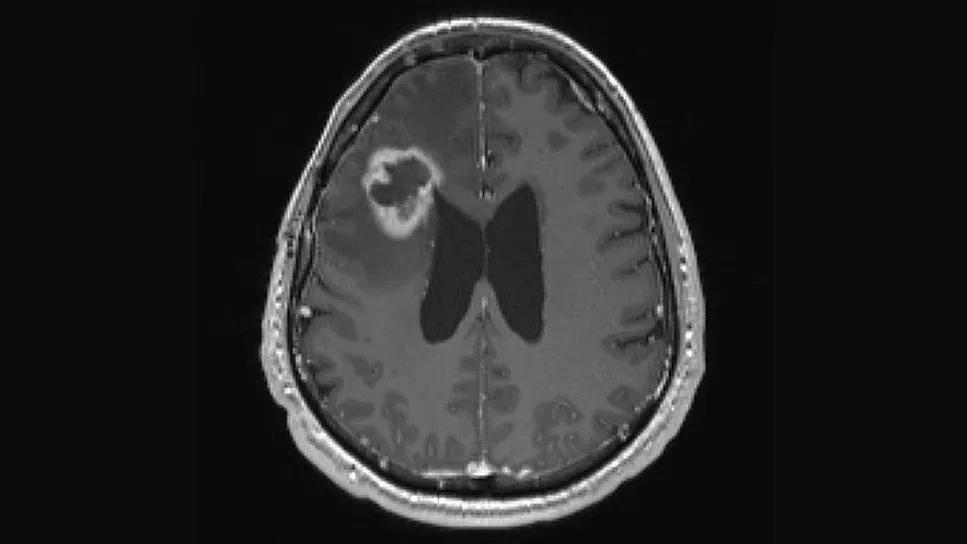
Beyond the core drug interventions, both trials incorporate advanced imaging techniques. Radiomic features extracted from MRI scans will be analyzed to identify potential biomarkers that predict treatment response. This move towards personalized medicine, tailoring treatment strategies based on individual tumor characteristics, represents a significant step forward in glioblastoma care.
Looking Ahead: The Future of Repurposed Therapies in Oncology
The Cleveland Clinic trials exemplify a growing trend in oncology: the strategic repurposing of existing drugs. This approach isn’t limited to glioblastoma; researchers are actively exploring similar strategies for other cancers, leveraging our growing understanding of tumor biology and the complex interplay between cancer cells and the immune system. The success of these trials could pave the way for a new era of faster, more affordable, and more effective cancer treatments.
Furthermore, the focus on modulating the tumor microenvironment – rather than solely targeting cancer cells – represents a fundamental shift in therapeutic strategy. By creating a more favorable environment for the immune system to function, we may unlock the potential of existing therapies and overcome the challenges of drug resistance. The convergence of drug repurposing, advanced imaging, and immunotherapeutic approaches holds immense promise for improving outcomes for patients with glioblastoma and beyond.
Frequently Asked Questions About Drug Repurposing in Glioblastoma
What are the advantages of drug repurposing compared to developing new drugs?
Drug repurposing significantly reduces the time and cost associated with bringing a new therapy to market. Existing drugs have already undergone extensive safety testing, streamlining the approval process.
How do methimazole and sitagliptin work in the context of glioblastoma?
Methimazole boosts hydrogen sulfide levels, which inhibits glioblastoma cell growth. Sitagliptin reduces the number of immunosuppressive cells (MDSCs), allowing the immune system to better attack the tumor.
What is the “window-of-opportunity” trial design?
This design allows researchers to administer therapies before surgery and then analyze the effects on the tumor microenvironment, providing valuable insights into drug mechanisms and potential biomarkers.
What are your predictions for the future of drug repurposing in cancer treatment? Share your insights in the comments below!
Discover more from Archyworldys
Subscribe to get the latest posts sent to your email.