
The pharmaceutical industry is obsessed with the “next big molecule,” but the real breakthrough in precision oncology might actually be a better inventory management system. For years, the race has been to invent new drugs for rare mutations—a process that is slow, prohibitively expensive, and often fails in clinical trials. However, new research from Gujral’s lab suggests we may already have the tools we need; we just haven’t been looking at them correctly.
- Expanded Utility: A comprehensive screen of 92 FDA-approved drugs increased the number of known kinase targets from 89 to 235.
- High Hit Rate: Existing drugs could potentially block 94% of cancer-driving kinase mutations and 97% of gene fusions.
- Strategic Repurposing: Drugs like tepotinib and gilteritinib are showing “off-label” efficacy against mutations they weren’t originally designed to target, providing a shortcut for treating rare cancers.
The Deep Dive: Moving Beyond the “Lock and Key”
To understand why this matters, you have to understand the “lock and key” philosophy of traditional drug design. Normally, a drug is developed to fit one specific “lock” (a kinase). If a cancer mutation changes the shape of that lock, the drug no longer works, and the patient is labeled “drug-resistant.” This has led to a cycle of desperate attempts to build a new key for every single single-point mutation found in the human population.
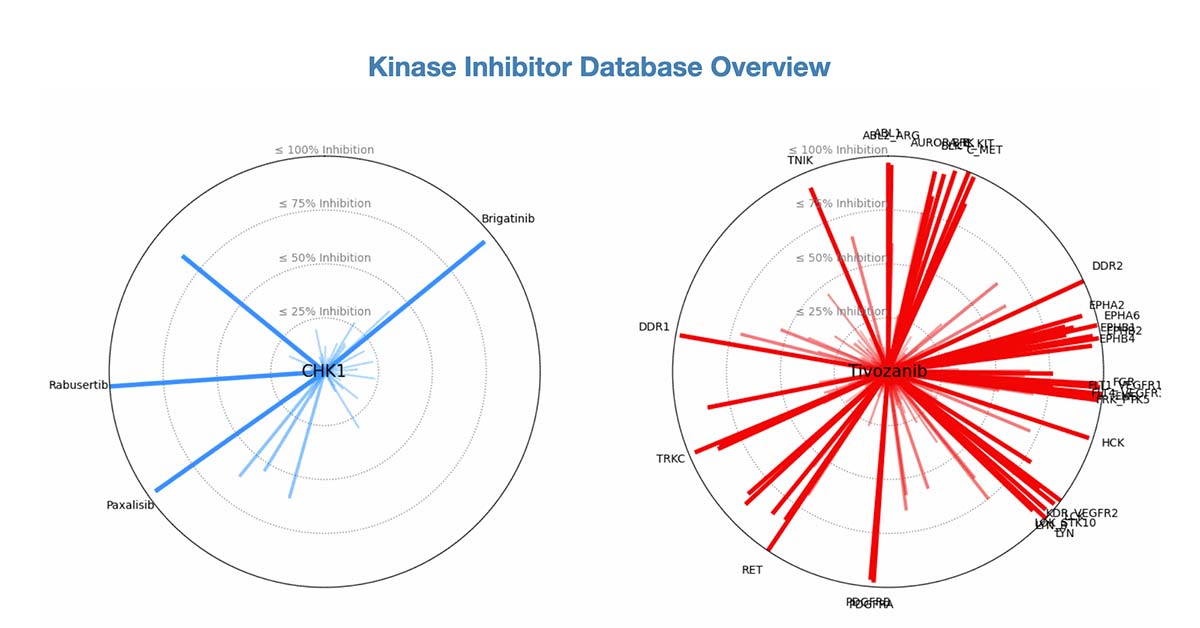
Gujral’s approach flips the script. By partnering with Reaction Biology to screen FDA-approved drugs against a massive library of 758 kinases—specifically focusing on the 349 mutant variants that actually drive tumor growth—the team discovered that many “keys” fit more “locks” than we thought. This is a classic case of latent utility: a drug designed for lung cancer (tepotinib) might be the perfect weapon for glioblastoma or even cardiovascular disease because it happens to block the IRAK1/4 kinase.
From a technical perspective, this is about efficiency. We are moving away from the hype of “miracle cures” and toward a data-driven mapping of existing chemical assets. The ability to use gilteritinib—a leukemia drug—to bypass resistance in lung cancer isn’t just a medical win; it’s a logistical masterstroke that bypasses a decade of R&D.
The Forward Look: Algorithm-Led Prescribing
The immediate future of oncology isn’t a new pill; it’s a better database. We should expect a shift toward “Algorithm-Led Prescribing,” where a patient’s specific mutant variant is sequenced and then matched against this expanded library of FDA-approved drugs rather than standard-of-care protocols.
However, the road to implementation has a significant bottleneck: regulatory inertia. The FDA approves drugs for specific indications. While the science shows that a drug can block a mutation, getting the legal and insurance framework to approve a “leukemia drug” for a “brain cancer” patient is a bureaucratic nightmare. Watch for a surge in “off-label” pilot studies and a push for new regulatory pathways that allow for drug repurposing based on kinase-mapping rather than traditional indication-based trials.
Ultimately, the goal is the “one-two punch” mentioned in the study—combining existing inhibitors to block both the primary driver and the escape route the cancer uses to become resistant. The toolkit is already in the cabinet; the challenge now is the courage to use the tools for things they weren’t originally labeled for.
Discover more from Archyworldys
Subscribe to get the latest posts sent to your email.